Cambridge Cancer Research Hospital
CHANGING THE WAY WE TREAT CANCER


FIND EARLY, TREAT BETTER



1 IN 2 PEOPLE WILL BE DIAGNOSED WITH CANCER IN THEIR LIFETIME
In 2020, globally there were
18.1 MILLION CASES


In 2040, that will increase to
28.4 MILLION CASES



The Cambridge Cancer Research Hospital (CCRH) is a new kind of cancer hospital.
Here, researchers will develop new ways of finding cancer at the earliest possible stage, so treatments such as surgery, chemotherapy, and radiation are far less likely to be needed. Where we cannot detect cancers earlier, personalised medicine will use the power of Big Data and AI to deliver more targeted and effective treatments.
“IMAGINE A FUTURE WHERE PEOPLE NEVER GET CANCER AS WE KNOW IT. A WORLD WHERE YOUR DOCTOR CAN ACCURATELY TEST FOR THE EARLY STAGES OF CANCER, WHERE YOU INTERVENE WITH TREATMENTS THAT ARE STRAIGHTFORWARD AND RELATIVELY NON-TOXIC—MAYBE EVEN MINOR SURGERY—AND THAT’S IT.”
Professor Richard Gilbertson,
Lead for the Cambridge Cancer Research Hospital, Li Ka-shing Chair of Oncology, Head of Department of Oncology, Director of the CRUK Cambridge Centre at the University of Cambridge
THE CAMBRIDGE CANCER RESEARCH HOSPITAL WILL CHANGE THE WAY WE TREAT CANCER BY HARNESSING THE POWER OF TWO NEW RESEARCH INSTITUTES.
The Institute for the Early Detection of Cancer is pioneering a new paradigm in cancer detection, carrying out transformative research to detect cancer early enough to cure it. To do this, wewill overcome the challenges of translating early detection advances from research into clinical practice. Our multidisciplinary approach including engineering and physics workshops, prototyping facilities, and biology labs, will enable us to advance and improve early detection.


The Hospital’s Institute for Integrated Cancer Medicine will be a working laboratory using Big Data to benefit individual patients. By harnessing the power of AI and machine learning, we can meaningfully extract, combine, and use insights from individual genetic, molecular, and imaging data. This will become a powerful tool for more personalised and effective treatment.


BY CHANGING THE WAY WE TREAT CANCER, WE CAN CHANGE MILLIONS OF LIVES FOR THE BETTER.
THE
HOSPITAL



THE CAMBRIDGE CANCER RESEARCH HOSPITAL WILL HAVE 24,500M2 OF SPACE
Where clinicians and cancer researchers are co-located with physicists, engineers, mathematicians and computational scientists, to create innovative approaches that will dramatically improve patient care.
There will be around 35 research and related staff at the new University of Cambridge institutes and another 21 PhD students once we’re at full capacity – that’s 50 to 60 researchers directly working within the building plus extra researchers around campus as a result of increased activity.
Facilities within the Institute for the Early Detection of Cancer and the Institute for Integrated Cancer Medicine will include:
wet laboratories to test and analyse biological samples, and dry laboratories to perform applied or computational analyses through creation of computer-generated models.
state-of-the-art computational laboratories, where dry lab scientists can work alongside clinicians
space for assessing the effectiveness and acceptability of new tests through clinical trials
on-site expertise in trial design, health economics and epidemiology.
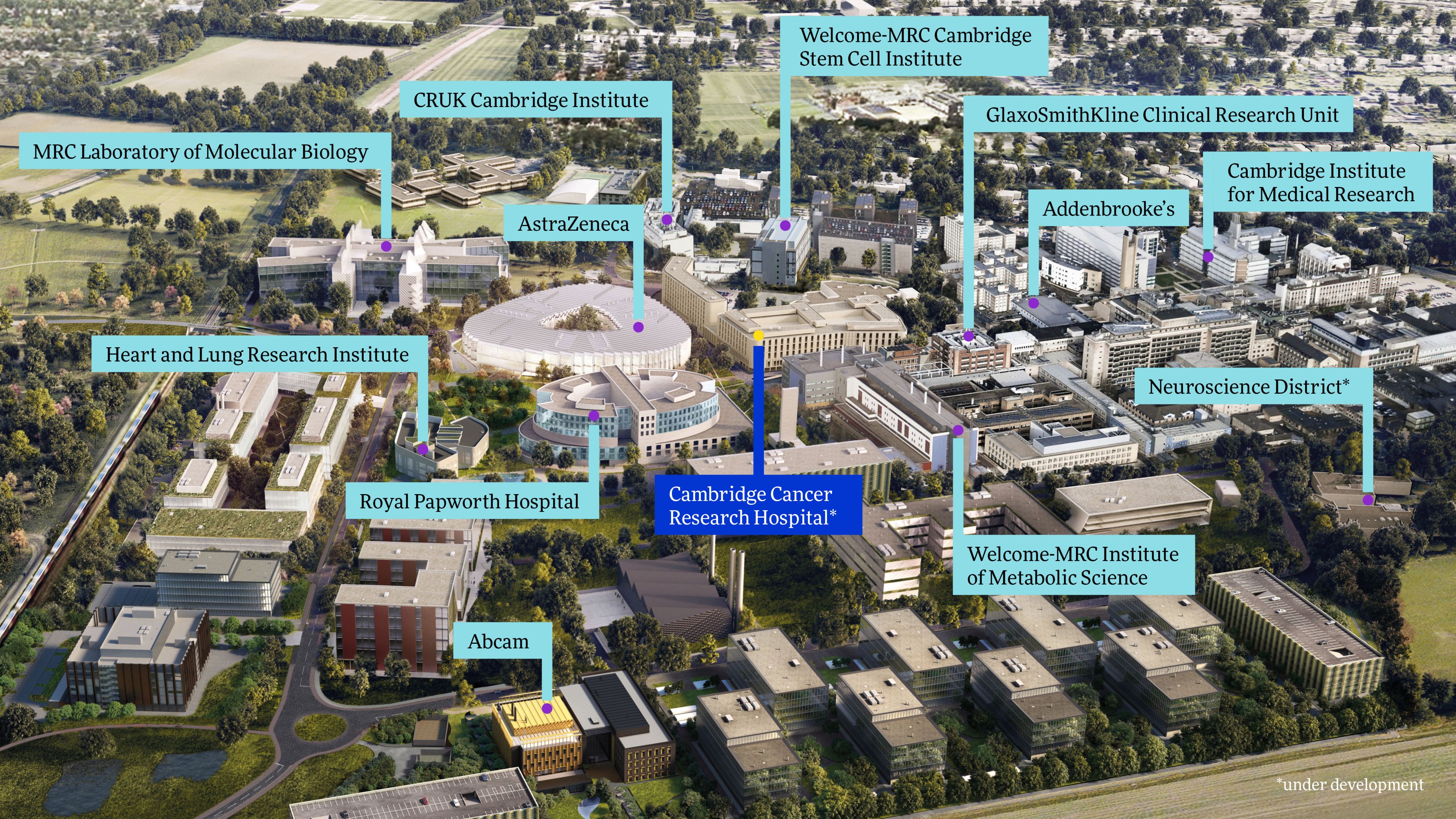
CCRH will be at the heart of Cambridge’s Biomedical Campus, the only bioscience ecosystem in Europe, and one of only four in the world.
Basic science through translational work will draw on the research efforts of nine world-leading research institutes, 24 University departments, and over 600 of the brightest minds working in health sciences.
Commercial partners, from University spin-outs and start-ups to AstraZeneca, will ensure what is developed here is delivered on a global scale.




GLOBAL
IMPACT


IN 2012, 65% OF ALL CANCER DEATHS WORLDWIDE OCCURRED IN LOW TO MIDDLE INCOME COUNTRIES. BY 2030, THIS IS PROJECTED TO INCREASE TO 75%.
TO DATE, CAMBRIDGE HAS MADE SOME OF THE MOST IMPORTANT AND EXCITING DEVELOPMENTS IN CANCER RESEARCH.





IN CAMBRIDGE, WE...
Discovered the structure of DNA and developed the technology (Next Generation Sequencing) to rapidly sequence the entire human genome
Pioneered the manufacture and use of monoclonal antibodies, a technology that now underpins routine cancer therapy globally
Identified numerous genetic abnormalities that drive the development and growth of multiple cancer types
Demonstrated that breast cancer has ten distinct sub-types, each with different drivers and prognoses
Invented numerous cancer drugs, including olaparib, a DNA repair inhibitor now regularly used to treat multiple types of cancer in women
Generated the first proof-of-principle that a simple blood test (liquid biopsy) can detect fragments of circulating tumour DNA, allowing for non-invasive, individualised snapshots of cancer development and recurrence
Determined the origins for two of the most common types of childhood brain tumours, and are now inventing new treatments
Spearheaded a revolutionary new imaging technology, which can reveal a tumour’s response to a drug within 24 to 48 hours of treatment
Developed the Cytosponge ‘pill on a string’ to detect Barrett’s oesophagus (the only known precursor to oesophageal adenocarcinoma), currently used by NHS Scotland
Cambridge spin-out Cyted has paved the way for AI to ease the burden of analysing Cytosponge samples, potentially reducing the diagnostic workload by 57%
Created a low-cost ‘cancer breathalyser’ that will determine whether volatile organic compounds from early lung cancer or other solid tumours can be found in a breath sample.
Developed PREDICT Breast and Prostate online tools, now helping patients in over 200 countries reach better clinical outcomes, avoid unnecessary treatments and experience less distress.
BREAKTHROUGH IDEAS DEVELOPED IN CAMBRIDGE HAVE CHANGED LIVES FOR THE BETTER IN EVERY CORNER OF THE WORLD.



EARLY
DETECTION
Within CCRH, the Institute for the Early Detection of Cancer will create, develop, and deliver new ways of finding cancer sooner.





A STAGE I CANCER DIAGNOSIS MEANS A LIKELY 80% SURVIVAL OF FIVE YEARS OR MORE, BUT A STAGE IV DIAGNOSIS REDUCES SURVIVAL TO A 10% CHANCE.
EXISTING EARLY DIAGNOSIS STRATEGIES ARE NOT SUCCEEDING.
FEWER THAN 10% OF ASYMPTOMATIC CANCERS ARE DETECTED.
The Institute for the Early Detection of Cancer will harness the power of Cambridge’s unique strengths in AI and novel diagnostics to translate research into clinical practice.
We are collaborating with some of the world’s best scientists in the International Alliance for Cancer Early Detection – a new flagship global partnership between the University of Cambridge, Cancer Research UK, the Canary Center at Stanford University, the Knight Cancer Institute at the Oregon Health and Science University in Portland, University College London and the University of Manchester.
The Institute will have a hotel space with engineering and physics workshops, prototyping facilities, and wet labs. Experts from around the world will come to Cambridge to iterate novel devices, prototypes, and technologies.
Healthy volunteers and patients will contribute data including genomic, and biomedical data along with detailed demographic and lifestyle information. Researchers will use this to inform cancer risk prediction and development of novel diagnostics and interventions. Within 10 years it will be a globally unique, national bioresource.





AT THE FOREFRONT OF INNOVATION
The Institute for the Early Detection of Cancer will harness the unique world-leading strengths of Cambridge – in biological, physical, mathematical, population and social sciences – to tackle the biggest challenges in early detection and translate these advances into clinical practice.
Our researchers are already making extraordinary progress.
A new way to identify tumours that could be sensitive to immunotherapies
Dr Serena Nik-Zainal developed an algorithm to identify tumours that could be sensitive to particular immunotherapies by using data from thousands of NHS cancer patient samples sequenced through the 100,000 Genomes Project. Her team identified nine DNA repair genes that are critical guardians of the human genome from damage caused by oxygen and water, as well as errors during cell division. The MMRDetect clinical algorithm identifies these tumours and then improves the personalisation of cancer therapies to exploit those weaknesses. The algorithm will be rolled out across all cancers picked up by Genomics England.
Finding cancer risk in the blood
Dr Jamie Blundell's team has addressed a key question in early detection: which mutations enable cells to expand most rapidly, and give the highest risk of cancer? Using blood-sequencing data from 50,000 people the team built a league table of the most pathogenic mutations in blood. This will shed light on how mutations drive the development of cancer and will help to accelerate the development of risk predictors.
Transforming innovation into commercial success
A University spin-out, Inivata, developed a simple but revolutionary blood test – or liquid biopsy – which uses genomics to help detect cancer, stratify patients and monitor individual responses to treatments. Its first product, InVisionFirst™-Lung is now commercially available for treating patients with advanced non-small cell lung cancer.
EARLY DETECTION IN ACTION: CYTOSPONGE
Cambridge’s early detection programme is led by Professor Rebecca Fitzgerald. Her ingenious invention – the Cytosponge – is a revolutionary and simple technique to diagnose Barrett’s oesophagus, a pre-cancerous condition that can increase the risk of developing oesophageal cancer.
Detecting and monitoring Barrett’s oesophagus requires repeated endoscopies – where patients are sedated and a camera on a flexible tube is passed down the throat. It is invasive, involved and expensive.
Fitzgerald’s idea is simple: a pill on a string that, when swallowed, expands into a small, rough-textured sponge. When pulled back up, it collects cells from the gullet. She won the prestigious Westminster Medal for her work.
However, Fitzgerald and her team needed an accurate and fast diagnostic test. Her team identified a protein that was present in the abnormal cells, and an antibody that could be applied to the cells. This test, known as the Cytosponge-TFF3 test (after the antibody, named Trefoil Factor 3) stains cells brown, allowing them to be easily identified, a process that has now been made quicker using artificial intelligence.
This test is 10 times more efficient than the standard diagnostic route, and is better at picking up early-stage oesophageal cancer. The procedure can be performed at a GP surgery by a trained nurse and is now used by NHS Scotland as standard treatment, and undergoing trials by NHS England.
A major bottleneck for scaling Cytosponge is the time it takes for a pathologist to analyse the samples. However, another Cambridge spin-out, Cyted, uses AI to speed up sample analysis. This alleviates pressure on the NHS, and increases the potential for Cytosponge to be adopted by health systems globally.
Researchers, guided by experienced pathologists, developed a semi-automated triage system. This meant that results for each sample were categorised into one of eight classes depending on sample quality and diagnostic clarity. Samples that were deemed to be low quality or more challenging for the AI were assessed manually by pathologists.
This triage system has proved successful and researchers believe that it could reduce Cytosponge-related workload for pathologists by 57%. Researchers believe the technology could, in the future, be applied to support the diagnosis of pancreatic, thyroid, and bowel cancer.
INTEGRATED
CANCER
MEDICINE
Where we cannot find cancer sooner, we will treat it better.




COST OF SEQUENCING A HUMAN GENOME.
THE INTEGRATED CANCER MEDICINE TEAM IS TRULY MULTIDISCIPLINARY:



WITH OVER 80 MEMBERS ACROSS 14 UNIVERSITY OF CAMBRIDGE DEPARTMENTS, CAMBRIDGE UNIVERSITY HOSPITALS AND INDUSTRY PARTNERS, SUCH AS GE HEALTHCARE AND NVIDIA.
THE COMBINED EXPERTISE AND RESOURCES IN GENETICS, IMAGING, BIG DATA AND AI ARE BEING DEPLOYED TO TREAT EACH PATIENT – AND EACH CANCER – INDIVIDUALLY, PREVENTING UNNECESSARY TREATMENTS AND SIDE EFFECTS.




TREATMENT BREAKTHROUGHS
Next-generation Whole Genome Sequencing
Medical oncologist Professor Jean Abraham and a team of AI experts have been working on an AI platform that integrates data such as samples, images, tests, and sequencing to enable analysis of complex data in real time. Next-generation sequencing technology allows tumours to be sequenced within 12 weeks – much quicker than usual. The results will ensure patients receive tailored treatment as well as identifying any genetic markers that could increase the chances of cancer in patients’ descendants.
Highly targeted biopsies
Cambridge researchers have developed a new advanced computing technique called radiomics that combines CT scans with ultrasound images to create a visual guide for doctors. This enables clinicians to create a tumour map, which is then superimposed on the ultrasound image of the tumour, and the combined image is used to guide the biopsy procedure. By taking targeted biopsies using this method, the research team reported that the diversity of cancer cells within the tumour was successfully captured, which is critical for selecting the best treatment. In future this technique could even replace clinical biopsies with ‘virtual biopsies’, sparing patients invasive procedures.
AI to improve cancer screening
Cambridge spin-out Lucida Medical is developing AI for cancer screening. Researchers developed software using radiogenomics, machine learning and image processing to analyse MRI scans. The technology helps to automate labour-intensive tasks such as marking out lesions, and avoid unnecessary invasive biopsies, with unprecedented accuracy and consistency. Lucida aims to screen up to 54 million men for prostate cancer each year using its technology, to offer the benefits of early detection and personalised care to everyone.
Simultaneous access to information
A collaboration between GE Healthcare, the University of Cambridge and Cambridge University Hospitals will integrate clinical, imaging, and genomic data from diagnosis through each treatment stage into a single cloud-based application. Using this, all medical teams – medical oncologists, clinical oncologists, surgeons, radiologists, pathologists and clinical nurse specialists – will have simultaneous access to the information needed to make faster, better-informed and highly personalised treatment decisions.
BREAST
UNIT
Integrated cancer medicine in action: Breast cancer.




BREAST CANCER IS THE MOST COMMON CANCER IN WOMEN WORLDWIDE.
THERE ARE MORE LOST DISABILITY-ADJUSTED LIFE YEARS (DALYS) BY WOMEN TO BREAST CANCER GLOBALLY THAN TO ANY OTHER TYPE OF CANCER.
OUR PERSONALISED BREAST CANCER PROGRAMME HAS ALREADY IDENTIFIED MULTIPLE IMPERCEPTIBLE MUTATIONS THAT ALLOWED US TO CHANGE PATIENT TREATMENT FOR THE BETTER.
This programme has set a new standard. It was the first group — worldwide — to use Cambridge-developed Next Generation Sequencing as a routine, standard-of-care diagnostic and clinical tool.
These data-led approaches are the key to unlocking better treatments, and we will implement them widely across all cancer types.
Predicting treatment and outcomes
Cambridge researchers developed PREDICT, a web-based tool that asks for some details about the patient and the cancer. It then uses data about the survival of similar women in the past to show the likely proportion of such women expected to survive up to fifteen years after their surgery with different treatment combinations. The PREDICT tool is now being used worldwide to improve targeting of treatment and better clinical outcomes.
International collaboration
The world’s most ambitious research to date on the role of heredity in breast cancer is being led by Professor Doug Easton, Director of the Centre for Cancer Genetic Epidemiology. 250 researchers from over 25 countries took part in the project and have pinpointed nine genes with solid evidence of involvement in the disease, which can now be targeted in genetic testing.
Tackling inequalities
Professor Charlotte Coles is leading a global commission – the Lancet Breast Cancer Commission – to change how breast cancer is treated around the world. By facilitating interdisciplinary, collaborative research, the project ultimately aims to tackle inequalities in breast cancer treatment by influencing global policy.
An international team of scientists, led by Cambridge researchers, has developed intricate maps of breast tumour samples, with a resolution smaller than a single cell. For the first time ever, they paired this imaging data with genomic data to create tumour ‘blueprints’. By matching these tumour images to individual patient data, researchers found that this technique could be used to predict how a patient's cancer might progress – and importantly – respond to different treatments.


SUPPORTING GLOBAL ADVANCES IN CANCER CARE
Excellence attracts excellence. Our research is changing the way we predict, diagnose and treat cancer across the world.
NOW WE NEED VISIONARY PHILANTHROPISTS TO SUPPORT OUR RESEARCHERS SO THEY CAN MAKE EVEN MORE OF THE BREAKTHROUGHS NECESSARY TO CURE CANCER.
The Cambridge Cancer Research Hospital will draw on the world-leading expertise found within the University and across the Biomedical Campus, to find cancer faster and treat it better.
New developments, including predictive tools, diagnostics, and treatments will be amplified, spreading out across our growing international network of collaborators so that new ideas reach the people who need them most.
We invite you to work with us to make this future a reality.
We are raising
£50 MILLION
to build the Cambridge Cancer Research Hospital and change the story of cancer, forever.
FOR MORE INFORMATION PLEASE CONTACT
Mary Jane Boland
Director of Development
Cambridge University Health Partners
University of Cambridge Development and Alumni Relations
+44 (0)7938 486966
maryjane.boland@admin.cam.ac.uk
1 Quayside, Bridge Street, Cambridge
CB5 8AB

